Thyroid Enlargement (Goiter): A Comprehensive Guide to Causes, Symptoms, and Treatment Options
The thyroid gland is a small, butterfly-shaped gland that plays a critically important role in the human body. It is located at the front of the neck just below the larynx and surrounds the trachea, acting as the main regulator of the body’s metabolic processes. It produces hormones that affect nearly every cell, tissue, and organ in the body, controlling heart rate, body temperature, weight, and energy levels.
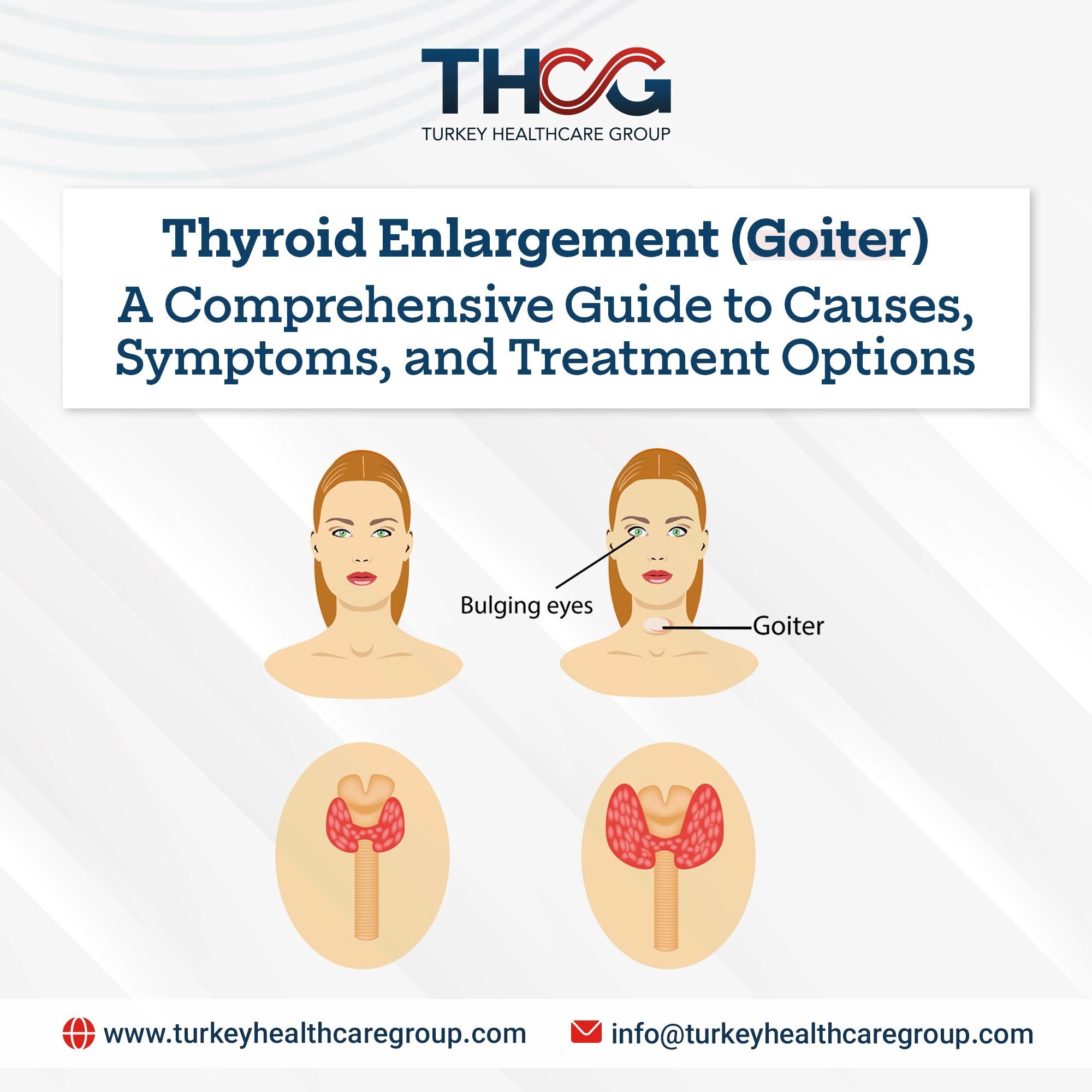
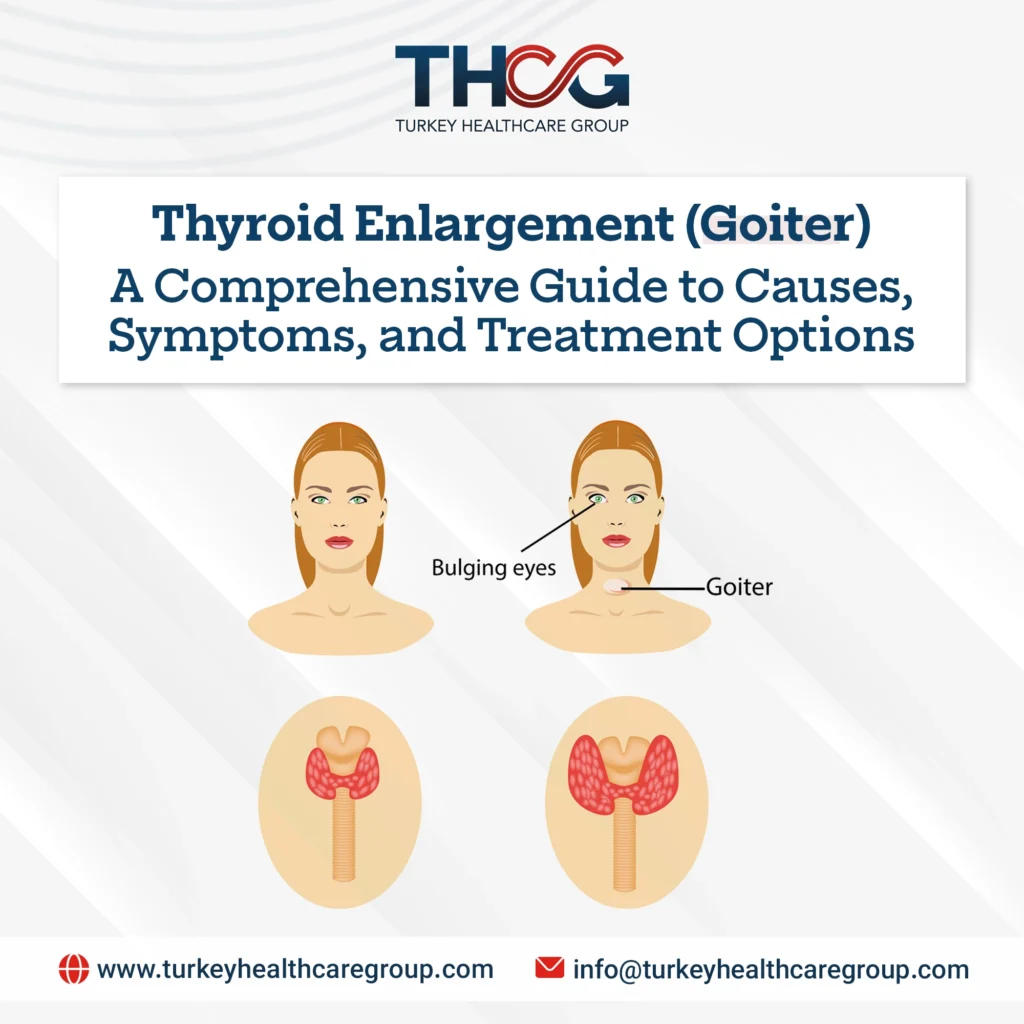
However, this vital gland is not immune to disorders. One of its most prominent and historically visible problems is known as thyroid enlargement (goiter), which is a swelling of the neck resulting from an enlarged thyroid gland.
Over the centuries, goiter has been a notable feature in art, literature, and medical history. Although it was once common in certain regions, medical advances have significantly reduced its prevalence. Nevertheless, goiter remains an important medical condition. It is not a disease in itself but a sign that may indicate a wide spectrum of thyroid disorders. At Turkey Healthcare Group, we believe that understanding thyroid enlargement is essential for appreciating the delicate balance of the endocrine system.
Thyroid Enlargement (Goiter)
A Comprehensive Guide to Causes, Symptoms, and Treatment OptionsThe thyroid gland is a small, butterfly-shaped gland that plays a critically important role in the human body. It is located at the front of the neck just below the larynx and surrounds the trachea, acting as the main regulator of the body’s metabolic processes. It produces hormones that affect nearly every cell, tissue, and organ in the body, controlling heart rate, body temperature, weight, and energy levels. However, this vital gland is not immune to disorders. One of its most prominent and historically visible problems is known as thyroid enlargement (goiter), which is a swelling of the neck resulting from an enlarged thyroid gland.
Over the centuries, goiter has been a notable feature in art, literature, and medical history, often serving as a clear visual indicator of nutritional or hormonal imbalance. Although it was once common in certain regions of the world, medical advances and public health initiatives have significantly reduced its prevalence in many countries. Nevertheless, goiter remains an important medical condition. It is not a disease in itself but a sign that may indicate a wide spectrum of thyroid disorders ranging from benign to serious. Understanding thyroid enlargement in terms of its causes, types, diagnosis, and treatment is essential for appreciating the delicate balance of the endocrine system and the profound impact that even a minor deficiency or disorder in this gland can have on human health.
What Is Thyroid Enlargement?
At its core, thyroid enlargement is not a disease in itself, but a physical sign indicating an underlying thyroid problem. It is defined as any abnormal increase in the size of the thyroid gland. It may appear as a noticeable swelling or be detected only during clinical examination. Enlargement may be diffuse, meaning the entire gland grows uniformly, or nodular, where nodules or lumps form within the gland. Thyroid enlargement may occur when hormone levels are normal (euthyroid), overactive (hyperthyroid), or underactive (hypothyroid).
The size of the enlargement varies greatly; it may be mild and detectable only by a physician, or large enough to visibly alter the shape of the neck. In very severe cases, the enlarged gland may compress the trachea or esophagus, causing difficulty breathing or swallowing, or even changes in the voice such as hoarseness. Importantly, the presence of enlargement does not necessarily mean there is a serious disease or abnormal thyroid hormone level.
Thyroid Gland Function
To properly understand thyroid enlargement, it is essential to first understand the gland’s structure and normal function. The gland lies in the front of the neck and consists of two lobes connected by a thin bridge of tissue known as the isthmus, giving it its characteristic butterfly shape. It contains millions of small follicles, which are the functional units of the gland and are filled with a protein substance known as colloid, serving as a reservoir for thyroid hormone components.
The primary role of the gland is to produce two main hormones: thyroxine (T4) and triiodothyronine (T3). These are the only hormones in the body that contain iodine, an essential mineral that the body cannot produce and must obtain from the diet. The production of these hormones is tightly regulated by the pituitary gland in the brain, which releases thyroid-stimulating hormone (TSH) to stimulate the thyroid to absorb iodine from the bloodstream and produce and release hormones into circulation.
T3 and T4 act as the “leaders of metabolism” in the body, controlling the rate of energy use, protein synthesis, and the body’s response to other hormones. They are also essential for brain development in children and for maintaining the health of the heart, digestive system, muscles, and bones. This system operates through a precise negative feedback loop: when hormone levels rise in the blood, the pituitary reduces TSH secretion, and when levels fall, TSH secretion increases to stimulate the thyroid.
Any disruption in this system, whether due to iodine deficiency, autoimmune disease, or developmental abnormalities can lead to thyroid enlargement as a compensatory response.
Causes of Thyroid Enlargement
The Main Cause: Iodine Deficiency
Iodine deficiency is the most common cause of thyroid enlargement worldwide. It is a clear example of how a simple nutritional deficiency can lead to a major physiological disorder. Iodine is essential for the formation of T3 and T4, and without it the gland cannot produce adequate amounts of these hormones.
When iodine levels drop, the pituitary gland responds by increasing TSH production to stimulate the thyroid to work harder. This continuous stimulation causes thyroid cells to enlarge and multiply (hyperplasia), leading to gradual enlargement of the gland in an attempt to absorb as much iodine as possible. Over time, this chronic stimulation results in a diffuse and smooth enlargement, the classic form of iodine-deficiency goiter.
Historically, goiter was common in inland regions where soil, food, and water were low in iodine, such as the Alps, the Himalayas, and the Great Lakes region of North America. These areas became known as “goiter belts.” The health and social impacts were significant, including visible deformities and, in severe iodine deficiency during pregnancy, intellectual disability in children known as cretinism.
The solution to this global health problem became one of the greatest public health achievements of the 20th century: iodization of table salt. This simple measure dramatically reduced goiter cases in countries that adopted it. Today, iodine deficiency is rare in countries with effective salt iodization programs, but it remains a major issue in regions lacking such initiatives, making it the leading cause of goiter globally.
Other Causes of Thyroid Enlargement
Although iodine deficiency remains the most common cause worldwide, other causes are more common in iodine-sufficient regions such as the United States, Europe, and many developed countries.
- Hashimoto’s Thyroiditis
This is the most common cause of thyroid enlargement (and hypothyroidism) in iodine-sufficient countries. It is an autoimmune disorder in which the immune system mistakenly attacks thyroid tissue, causing chronic inflammation and gradual destruction of thyroid cells.
In early stages, inflammation may cause thyroid enlargement, appearing as a visible or palpable swelling in the neck. Over time, hormone production gradually declines due to tissue damage, leading to hypothyroidism. The enlargement in this condition is typically firm, smooth, and painless.
- Graves’ Disease
This is the most common cause of hyperthyroidism and is also an autoimmune disorder. The body produces abnormal antibodies called thyroid-stimulating immunoglobulins (TSI) that mimic TSH and continuously overstimulate the thyroid gland, causing enlargement and excessive hormone production.
Thyroid enlargement in Graves’ disease is typically soft and diffuse and is often associated with distinctive symptoms such as:
• Protruding eyes (thyroid eye disease)
• Skin changes such as thickening of the skin on the shins, known as pretibial myxedema
- Thyroid Nodules
With aging, lumps or nodules may form in the thyroid due to abnormal cell growth. These nodules are very common, and studies suggest that up to 50% of people over the age of 60 have at least one thyroid nodule.
Most nodules are benign and asymptomatic, but when they grow large, they may cause visible neck enlargement known as nodular goiter.
• A single nodule: Uninodular goiter
• Multiple nodules: Multinodular goiter
In some cases, certain nodules produce hormones independently of the body’s control, causing hyperthyroidism, a condition known as toxic multinodular goiter.
- Thyroid Cancer
Goiter is rarely the first sign of thyroid cancer, but the presence of a single hard, fixed, rapidly growing mass may indicate malignancy.
Cancer-related enlargement is usually asymmetrical and may be associated with:
• Enlarged lymph nodes in the neck
• Hoarseness
• Difficulty swallowing
- Other Less Common Causes
• Viral thyroiditis causing temporary inflammation and enlargement
• Certain medications such as lithium used to treat bipolar disorder
• Temporary hormonal changes during puberty or pregnancy that may cause mild, temporary enlargement
Goiter Classification
Goiter can be classified in several ways to facilitate diagnosis and treatment.
First: By Structure
• Diffuse goiter: Uniform enlargement of the entire gland (as in Graves’ disease or early iodine deficiency).
• Nodular goiter: Enlargement due to one or more nodules.
- Uninodular
- Multinodular
Second: By Function
• Euthyroid goiter: Enlarged gland with normal hormone production.
• Hyperthyroid goiter: Enlarged gland producing excessive hormones (as in Graves’ disease).
• Hypothyroid goiter: Enlarged gland producing insufficient hormones (as in Hashimoto’s thyroiditis).
Third: By Size
• Grade 0: No enlargement; gland not palpable or visible.
• Grade 1: Palpable enlargement but not visible in the normal neck position.
• Grade 2: Palpable and visible enlargement in the normal neck position.
• Grade 3: Very large enlargement visible from a distance and may cause breathing or swallowing difficulties.
Symptoms of Thyroid Enlargement and When to See a Doctor
In many cases, small enlarged thyroid glands cause no symptoms at all and are discovered incidentally during a routine medical examination or imaging study (such as a CT scan) performed for another reason.
The most obvious sign of thyroid enlargement is swelling or a lump at the front of the neck. As the enlargement increases in size, it may begin to cause local compressive symptoms due to its proximity to the trachea and esophagus. These symptoms include:
• A feeling of tightness or pressure in the throat
• Persistent cough that does not resolve
• Hoarseness or changes in voice tone
• Difficulty swallowing (especially solid foods)
• Difficulty breathing, which may worsen when lying down or raising the arms
• Visible swelling that moves up and down أثناء swallowing
In addition to these local symptoms, signs related to thyroid dysfunction may appear:
Symptoms of Hyperthyroidism (in toxic goiter)
Unexplained weight loss, rapid or irregular heartbeat, anxiety, tremors, heat intolerance, excessive sweating, and general fatigue.
Symptoms of Hypothyroidism (in Hashimoto’s thyroiditis)
Weight gain, fatigue and lethargy, cold intolerance, constipation, dry skin, depression, and muscle pain.
You should consult a doctor immediately if any neck swelling appears, or if you experience difficulty breathing or swallowing, or any signs of thyroid hormone imbalance. Early diagnosis helps identify the exact cause and establish an appropriate treatment plan before the condition worsens.
Diagnosis of Thyroid Enlargement
The diagnostic process begins with a detailed medical history and physical examination.
The doctor will ask about symptoms, family history of thyroid disease, dietary habits (especially iodine intake), and medications used.
During the examination, the physician will palpate the neck to assess the size, shape, texture, and movement of the gland, and check for lumps, nodules, or enlarged lymph nodes.
Based on this initial assessment, the doctor may request several tests to determine the cause precisely:
- Thyroid Function Tests (Blood Tests)
These are the cornerstone of diagnosis.
Blood tests measure TSH, free T4, and sometimes T3 levels.
The results show whether the thyroid is functioning normally, overactive, or underactive, helping guide the physician toward the likely cause. - Antibody Tests
If an autoimmune disease such as Hashimoto’s or Graves’ disease is suspected, antibody tests are performed, including:
• Thyroid peroxidase antibodies (TPO Ab) in Hashimoto’s thyroiditis
• TSH receptor antibodies (TRAb) in Graves’ disease - Ultrasound Imaging
A painless, noninvasive test that uses sound waves to create a detailed image of the thyroid.
It helps determine whether the enlargement is diffuse or nodular, evaluates gland size and nodule characteristics, and shows whether nodules are solid or fluid-filled.
It also helps determine whether a fine-needle biopsy is needed. - Fine-Needle Aspiration (FNA) Biopsy
If a suspicious nodule is detected on ultrasound, a small sample of cells is taken using a thin needle and examined in the laboratory.
This is the most accurate method for determining whether a nodule is benign or malignant. - Thyroid Scan (Radioactive Iodine Uptake Test)
Used in selected cases to evaluate hyperthyroidism.
The patient receives a small dose of radioactive iodine or technetium, and images are taken to assess uptake patterns.
This test helps differentiate between:
• Graves’ disease: diffuse high uptake throughout the gland
• Toxic nodules: a “hot” area with increased uptake and reduced activity in the rest of the gland
Treatment of Thyroid Enlargement
Treatment depends entirely on the underlying cause, the size of the enlargement, and its effect on breathing, swallowing, or thyroid function. There is no single treatment suitable for all patients.
- Observation and Monitoring
For small enlargements that cause no symptoms and have normal thyroid function, periodic monitoring through clinical exams and ultrasound is usually sufficient to ensure stability. - Iodine Supplementation
When iodine deficiency is present, treatment is simple: restoring iodine intake.
This can be achieved by:
• Eating iodine-rich foods such as seafood, dairy products, and eggs
• Taking iodine supplements and using iodized salt
The enlargement often shrinks gradually after nutritional balance is restored. - Thyroid Hormone Replacement Therapy
This is the primary treatment for goiter caused by Hashimoto’s thyroiditis.
Patients receive synthetic thyroid hormone (Levothyroxine) daily to normalize hormone levels and treat hypothyroidism.
This therapy also suppresses TSH secretion, reducing stimulation of the gland and helping the goiter shrink over time. - Antithyroid Medications
In Graves’ disease or toxic multinodular goiter, medications such as:
• Methimazole
• Propylthiouracil
These drugs reduce hormone production. Beta-blockers may also be prescribed to quickly control symptoms such as palpitations and tremors.
However, these medications rarely reduce goiter size permanently. - Radioactive Iodine Therapy (RAI)
An effective and definitive treatment for hyperthyroidism.
The patient takes a calculated dose of radioactive iodine (I-131), which is absorbed by overactive thyroid cells, gradually destroying them and shrinking the gland over weeks or months.
A major side effect is the frequent development of permanent hypothyroidism, requiring lifelong hormone replacement therapy. - Surgery (Thyroidectomy)
Partial or total thyroid removal may be required in the following situations:
• Large goiter causing compression of the trachea or esophagus
• Enlargement that continues to grow despite treatment
• Suspicious or confirmed cancerous nodules
• Multinodular goiter causing cosmetic deformity
• Certain cases of Graves’ disease not responsive to medication or radioactive iodine
Types of surgery depend on the case:
• Lobectomy (removal of one lobe)
• Subtotal thyroidectomy
• Total thyroidectomy
After total thyroid removal, lifelong thyroid hormone replacement therapy is required.
Living with Thyroid Enlargement and the Importance of Regular Follow-Up
For many patients, thyroid enlargement is a chronic condition that can be easily managed. The key to successful treatment lies in a close and cooperative relationship with a specialist physician, most often an endocrinologist who specializes in hormonal disorders.
Regular follow-up is essential to evaluate the size of the enlargement, ensure that hormone levels remain within the optimal range, and adjust treatment when necessary. Patients who take thyroid hormone replacement therapy should undergo periodic TSH testing, as the required dose may change over time due to aging, weight changes, or the use of other medications.
Patients who have undergone radioactive iodine therapy or thyroid surgery require lifelong follow-up. Even in mild cases that do not require active treatment, an annual medical check-up remains a wise step to ensure stability and prevent progression.
Thyroid enlargement represents a scientific and human journey that connects geography, nutrition, immunity, and endocrinology. From being a widespread condition in iodine-deficient regions to becoming a clinically manageable sign today, goiter reflects the remarkable progress of public health and medical knowledge.
Although neck swelling may be a source of concern for patients, it is important to remember that thyroid enlargement is not a disease in itself, but a symptom indicating an underlying disorder. In an era with precise diagnostic tools and multiple effective treatment options, most cases can be successfully controlled, allowing patients to live fully normal and healthy lives.
The thyroid gland’s search for iodine, its susceptibility to autoimmune conditions, and its tendency to form nodules all remind us that our bodies function within a delicate and complex hormonal balance. Thyroid enlargement remains a visible symbol of this hidden biological harmony and a reminder of the importance of maintaining balance for long-term health and well-being.
With early detection, regular follow-up, and adherence to personalized treatment, this condition can be understood and effectively controlled, minimizing its impact on quality of life.
Living with Thyroid Enlargement and the Importance of Regular Follow-Up
For many patients, thyroid enlargement is a chronic condition that can be easily managed through a cooperative relationship with an endocrinologist. Regular follow-up ensures that hormone levels remain within the optimal range. Patients can easily manage their appointments and check-ups via our Online Services.
With early detection, regular follow-up, and adherence to personalized treatment at Turkey Healthcare Group, this condition can be understood and effectively controlled. You can learn more about our surgical success stories and progress in our Achievements and Medical Articles and our Media Center.
Frequently Asked Questions (FAQs) About Thyroid Enlargement (Goiter)
1. What is thyroid enlargement (goiter)?
A goiter is an abnormal enlargement of the thyroid gland, which is the butterfly-shaped gland located at the front of the neck. It is a sign of an underlying thyroid issue, not a specific disease.
2. Does having a goiter mean I have thyroid cancer?
No, the vast majority of goiters and thyroid nodules are benign (non-cancerous). However, a rapid-growing or hard nodule requires medical evaluation to rule out cancer.
3. What is the primary function of the thyroid gland?
The thyroid gland is the master regulator of your body’s metabolism, controlling how your body uses energy, regulates heart rate, and manages body temperature.
4. What hormones does the thyroid gland produce?
It primarily produces thyroxine (T4) and triiodothyronine (T3). The production of these hormones is controlled by TSH (Thyroid-Stimulating Hormone) from the pituitary gland.
5. What is the most common cause of a goiter worldwide?
Globally, a lack of iodine in the diet is the most common cause of thyroid enlargement. The gland swells as it works harder to absorb whatever little iodine is available.
6. What is Hashimoto’s Thyroiditis?
It is an autoimmune disorder where the immune system attacks the thyroid, causing inflammation, gradual destruction of the gland, hypothyroidism, and a firm, painless goiter.
7. What is Graves’ disease?
Graves’ disease is an autoimmune condition that causes the thyroid to become overactive (hyperthyroidism). It often results in a soft, diffuse goiter and sometimes protruding eyes.
8. Can thyroid nodules cause a goiter?
Yes. As people age, benign lumps or nodules can form in the thyroid. If multiple nodules grow, they cause a visibly enlarged neck, known as a multinodular goiter.
9. Is thyroid enlargement always visible from the outside?
No. Small goiters (Grade 1) are often only detectable when a doctor palpates (feels) your neck during a physical exam.
10. What are the physical symptoms of a large goiter?
A very large goiter can compress the windpipe or esophagus, causing difficulty swallowing, breathing issues (especially when lying down), a feeling of tightness, hoarseness, and persistent coughing.
11. What are the symptoms of an overactive thyroid (hyperthyroidism)?
Symptoms include unexplained weight loss, rapid heartbeat, tremors, anxiety, excessive sweating, and heat intolerance.
12. What are the symptoms of an underactive thyroid (hypothyroidism)?
Symptoms include unexplained weight gain, chronic fatigue, cold intolerance, dry skin, constipation, and muscle pain.
13. How do doctors diagnose the cause of a goiter?
Diagnosis usually involves a physical exam, blood tests (to measure TSH, T3, T4, and antibodies), and imaging like an ultrasound.
14. When is a Fine-Needle Aspiration (FNA) biopsy needed?
An FNA biopsy is performed if an ultrasound detects a suspicious or unusually large nodule inside the thyroid gland, to safely test the cells for cancer.
15. Does a goiter always require medical treatment or surgery?
No. If the goiter is small, hormone levels are normal, and it causes no breathing/swallowing issues, doctors may simply recommend periodic observation and monitoring.
16. How is an iodine-deficiency goiter treated?
It is treated by restoring iodine intake through the diet (eating seafood and using iodized salt) or taking specific iodine supplements prescribed by a doctor.
17. What is Thyroid Hormone Replacement Therapy?
It is the primary treatment for Hashimoto’s and hypothyroidism. Patients take daily synthetic thyroid hormones (Levothyroxine) to normalize levels and help shrink the goiter.
18. How does Radioactive Iodine Therapy (RAI) work?
Used for hyperthyroidism, the patient swallows a small dose of radioactive iodine, which is absorbed specifically by the thyroid, slowly destroying the overactive cells and shrinking the goiter.
19. When is surgery (Thyroidectomy) recommended?
Surgery is advised if the goiter is so large it causes breathing/swallowing difficulties, if thyroid cancer is suspected, or if hyperthyroidism doesn’t respond to other treatments.
20. Why choose Turkey Healthcare Group for thyroid treatment?
We provide comprehensive endocrinology care, advanced diagnostic imaging, and highly skilled endocrine surgeons capable of performing state-of-the-art partial or total thyroidectomies.
Turkey Healthcare Group stands out with a team of distinguished medical experts in Turkey, who always strive to provide the best healthcare services to patients.
If you are looking for exceptional healthcare or need medical consultation from top doctors, feel free to contact us.
We also invite you to view our leading medical staff and get to know their qualifications and experiences up close.
We are here to ensure you receive the best possible healthcare.