A comprehensive guide to Multiple Sclerosis (MS). Learn about its types (RRMS, PPMS), causes, symptoms, and the latest treatments at Turkey Healthcare Group.
Multiple Sclerosis (MS): Recent Advances in Diagnosis, Treatment, and Comprehensive Care
What Is Multiple Sclerosis (MS)?
Multiple sclerosis is an autoimmune and neurodegenerative disease that affects the central nervous system (CNS), which includes the brain, spinal cord, and optic nerves.
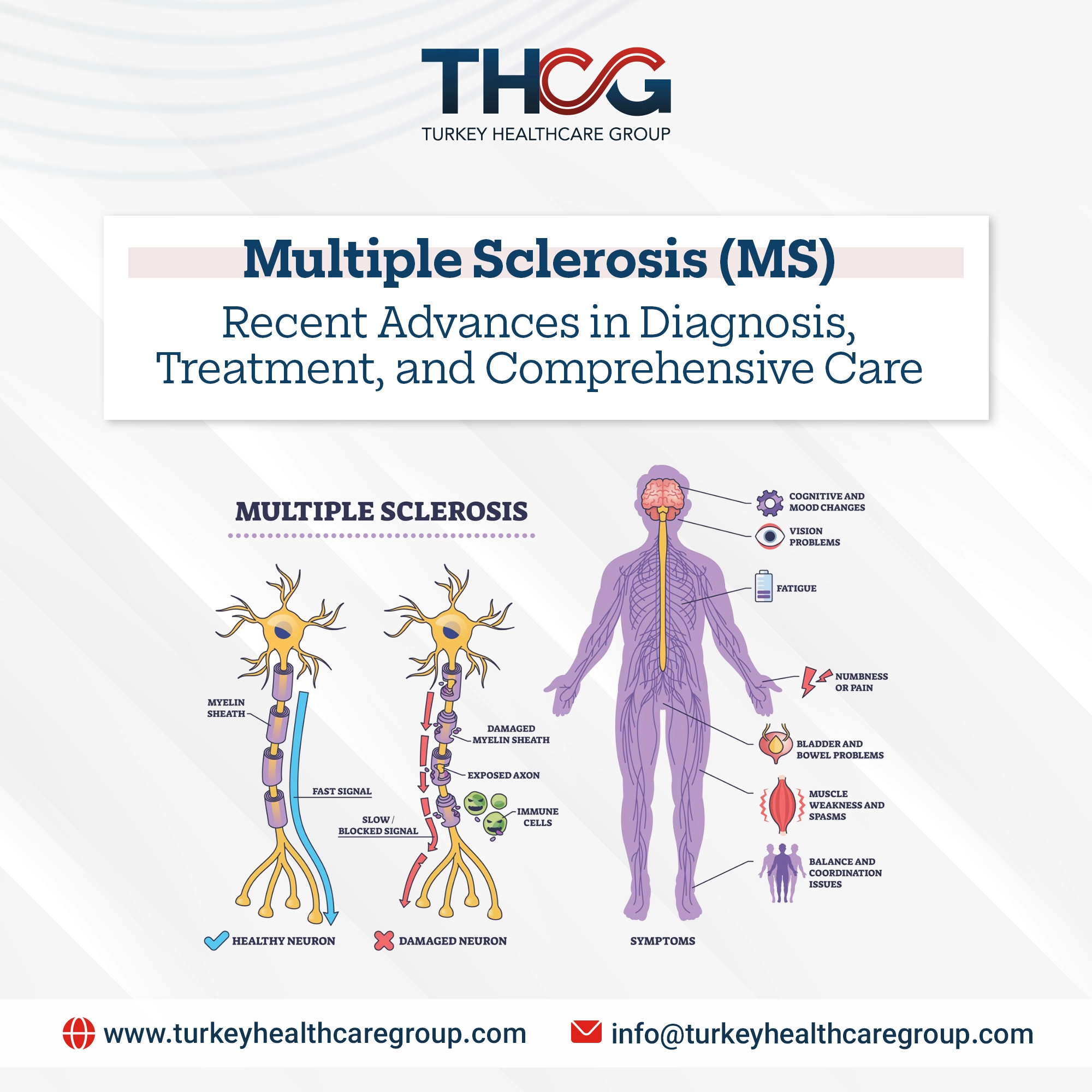
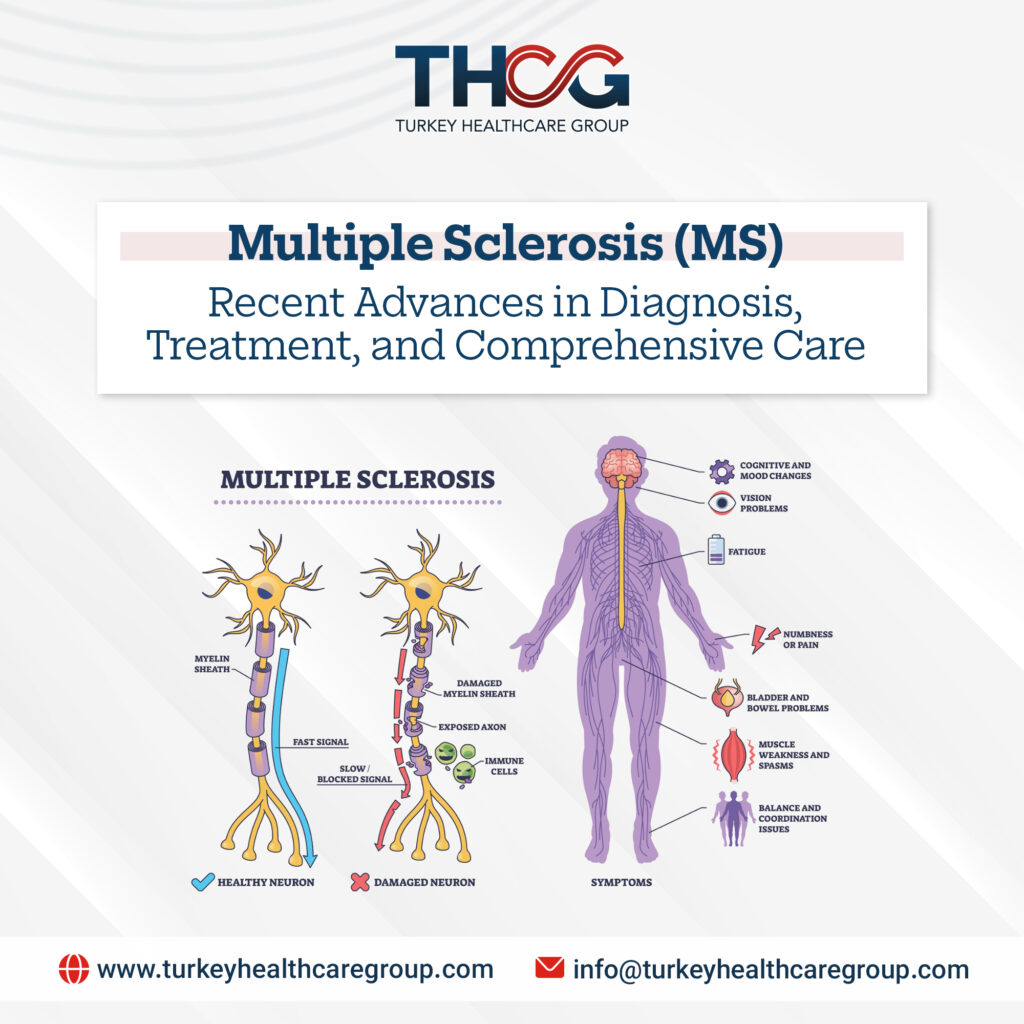
In a healthy person, nerve fibers (axons) are covered by a protective fatty layer called myelin. Myelin works like insulation on electrical wires, allowing nerve signals to travel quickly and efficiently from the brain to the rest of the body.
In MS, the immune system mistakenly attacks myelin, treating it as a foreign substance. This process is known as demyelination, which damages and eventually destroys the myelin sheath. As a result, nerve signals become distorted, slowed, or even completely blocked.
Over time, the nerve fibers themselves may become damaged or severed, a process known as neurodegeneration, which is the main cause of the long-term progressive disability often associated with MS.
The term “multiple sclerosis” literally means “multiple scars,” referring to the scarred plaques (sclerosis) that form in the CNS at sites of damage. These lesions are the hallmark findings seen on MRI scans.
Different Types of Multiple Sclerosis
MS is not a single-pattern disease. Its course, symptoms, and severity vary from person to person. Our expert neurologists classify it into four main clinical types to help predict progression and guide treatment.
1. Relapsing-Remitting MS (RRMS)
- Prevalence: The most common form, affecting about 85% of patients at initial diagnosis.
- Characteristics: Clearly defined relapses (attacks or flare-ups) followed by periods of remission or recovery.
- Relapse: A period of new or worsening neurological symptoms lasting at least 24–48 hours, not caused by fever or infection (which can cause a pseudo-relapse).
- Remission: Symptoms partially or completely improve, and the disease is not actively progressing, although some disability may remain.
- Progression: The disease does not steadily worsen between relapses, but accumulated damage over time can lead to increasing disability.
2. Secondary Progressive MS (SPMS)
- Prevalence: Many people with RRMS transition to SPMS after 10–25 years.
- Characteristics: The disease begins to progress steadily, with or without relapses or periods of mild improvement. The key feature is gradual worsening of neurological function and disability.
- Active or inactive: SPMS can be classified as active (with relapses or new MRI activity) or inactive, and as with progression or without progression.
3. Primary Progressive MS (PPMS)
- Prevalence: Affects about 10–15% of people with MS.
- Characteristics: From the beginning, there is continuous and gradual worsening of neurological function without clear relapses or remissions. However, temporary stability or mild improvement may occur.
- Active or inactive: Like SPMS, PPMS may be described as active (new MRI activity or occasional relapse) or inactive.
4. Clinically Isolated Syndrome (CIS)
- Definition: A first episode of neurological symptoms lasting at least 24 hours caused by inflammation and demyelination in the CNS. It may represent an early stage of MS.
- Importance: Not everyone with CIS develops MS, but the risk is higher if MRI shows lesions typical of the disease. CIS is often considered the earliest clinical stage of MS.
Understanding your MS type is the first step toward building an effective, personalized treatment and management plan.
What Causes Multiple Sclerosis?
The exact cause of MS is still not fully known, but research shows it is not caused by a single factor. It is believed to result from a complex interaction between genetic susceptibility and environmental triggers.
1. Autoimmune Link
The leading theory is that MS is an autoimmune disease. Normally, the immune system attacks viruses and bacteria to protect the body. In MS, immune cells (T and B cells) mistakenly cross the blood-brain barrier—which normally protects the brain—and launch an inflammatory attack on myelin and eventually on nerve fibers.
2. Genetic Susceptibility
MS is not strictly hereditary, but it tends to run in families.
- Risk in the general population: 0.1–0.2%
- Identical twin of an affected person: 25–30%
- Non-identical twin or sibling: 3–5%
This suggests that certain genes increase susceptibility, but they are not the sole cause. More than 200 genetic variants have been linked to increased MS risk.
3. Environmental Triggers
- Geographic location & sunlight exposure: MS is much more common in regions farther from the equator. This led researchers to study the role of sunlight and vitamin D, which helps regulate the immune system. Low vitamin D levels have repeatedly been linked to a higher MS risk.
- Epstein–Barr Virus (EBV): Growing scientific evidence shows a strong association between prior EBV infection (which causes infectious mononucleosis) and later development of MS. EBV is now considered a necessary but not sufficient factor for most MS cases, possibly priming the immune system for autoimmune attack.
- Smoking: Smoking is a major modifiable risk factor. It increases both the risk of developing MS and the likelihood of faster disease progression and greater disability.
- Adolescent obesity: Studies suggest that obesity during adolescence—especially in girls—is linked to a higher risk of developing MS later in life.
Overall, MS likely begins when environmental factors interact with a person’s genetic makeup, triggering the immune system to attack myelin.
What Are the Symptoms of Multiple Sclerosis (MS)?
Because MS can damage any part of the central nervous system, its symptoms are highly variable and differ from person to person in type and severity. Symptoms may be mild, moderate, or severe, and either temporary or permanent.
They often appear as relapses or flare-ups in relapsing-remitting MS (RRMS), or gradually worsen over time in progressive forms of the disease. Below is a detailed overview of the most common MS symptoms treated in our neurology departments.
1. Fatigue
One of the most common and disabling symptoms, affecting about 80% of patients. This is not ordinary tiredness, but a profound exhaustion that is disproportionate to activity and does not improve with rest.
2. Vision Problems
Often among the earliest signs of MS.
- Optic neuritis: Pain with eye movement, blurred vision, reduced color vision (colors appear faded), or temporary vision loss in one eye.
- Diplopia (double vision): Due to poor coordination of eye muscles.
- Nystagmus: Rapid, involuntary eye movements.
3. Numbness and Tingling
A common early symptom, often described as pins and needles, tightness, or pressure around the torso (known as the “MS hug”). Usually affects the face, arms, legs, or trunk.
4. Muscle Weakness, Spasticity, and Mobility Problems
- Muscle weakness: Often affects the legs and makes walking difficult.
- Spasticity: Muscle stiffness or painful involuntary spasms that interfere with movement, sleep, and daily activities.
- Balance and walking problems: Damage to the cerebellum or spinal cord may cause coordination issues and an unsteady gait.
5. Bladder and Bowel Dysfunction
Common but often under-discussed.
Bladder issues:
- Urgency or frequent urination
- Difficulty starting urination
- Urinary incontinence
- Incomplete bladder emptying
Bowel issues:
- Constipation (most common)
- Occasionally bowel incontinence
6. Sexual Dysfunction
Nerve damage can affect sexual arousal and response in both men and women, often due to a combination of physical and psychological factors.
7. Cognitive Changes
About 50% of people with MS experience some degree of cognitive impairment, usually mild but impactful on daily life. Examples include:
- Short-term memory problems
- Difficulty concentrating and processing information
- Challenges with planning, problem-solving, and finding words while speaking
8. Emotional Changes and Depression
Living with a chronic illness and damage to mood-regulating brain areas make depression and anxiety more common in MS. Some patients may experience pseudobulbar affect, which causes uncontrollable episodes of laughing or crying.
9. Pain
Both acute and chronic pain are common in MS.
- Neuropathic pain: Burning, stabbing, or tingling sensations caused by nerve damage.
- Musculoskeletal pain: From spasticity or abnormal walking.
- Headaches: Also common in some patients.
10. Speech and Swallowing Difficulties
In later stages, patients may develop:
- Dysarthria: Slurred or slow speech
- Dysphagia: Difficulty swallowing
Having one or even several of these symptoms does not necessarily mean MS, as they can occur in many other conditions. However, persistent or unexplained neurological symptoms should be evaluated by a medical professional for proper diagnosis.
How Is Multiple Sclerosis Diagnosed?
There is no single test that can definitively diagnose multiple sclerosis. Because its symptoms can resemble many other neurological disorders, diagnosis relies on ruling out other causes and finding evidence consistent with the known mechanisms of MS. Neurologists at our hospitals usually use a combination of the following:
1. Detailed Medical History and Neurological Examination
The doctor asks about symptoms, when they began, how long they last, and their severity. A comprehensive neurological exam evaluates vision, muscle strength, coordination, balance, reflexes, and sensation, looking for signs of damage in the central nervous system (CNS).
2. Magnetic Resonance Imaging (MRI)
MRI is the most important tool for diagnosing MS. It can detect characteristic lesions (plaques or scars) in the brain and spinal cord using the latest medical technologies.
MRI helps determine:
- Whether damage is present in multiple areas of the CNS (dissemination in space)
- Whether lesions appeared at different times (dissemination in time)
These two principles form the basis of the modern McDonald Criteria for diagnosing MS.
3. Lumbar Puncture (Spinal Tap)
In some cases, a sample of cerebrospinal fluid (CSF) is collected from the lower back and analyzed for:
- Oligoclonal bands: Abnormal immune proteins found in the CSF of more than 90% of people with MS, indicating immune activity within the CNS.
4. Evoked Potentials Tests
These tests measure electrical activity in the brain in response to specific stimuli and can detect slowed nerve signal transmission, even in areas without obvious symptoms.
Types include:
- Visual Evoked Potentials (VEP): Most common; measures brain response to visual stimuli.
- Somatosensory Evoked Potentials (SSEP): Response to electrical stimulation of arms or legs.
- Brainstem Auditory Evoked Potentials (BAEP): Response to sound stimuli.
These steps also help rule out similar conditions such as Lyme disease, Lupus, Vitamin B12 deficiency, and certain genetic disorders.
How Is Multiple Sclerosis Treated?
Although there is no cure yet, the treatment landscape for MS has changed dramatically over the past three decades. You can read more about recent medical breakthroughs in our Medical Articles section.
Today, many therapies aim to control disease activity, slow progression, treat relapses, and manage symptoms. This allows most people with MS to live long, active, and high-quality lives.
1. Disease-Modifying Therapies (DMTs)
These medications are the cornerstone of MS treatment, especially for RRMS, active SPMS, and CIS.
Main goals:
- Reduce relapse frequency and severity
- Decrease new MRI lesion formation
- Slow disability progression over time
More than 20 FDA-approved medications exist, categorized by how they are given: Injectable therapies, Oral medications, and Intravenous infusions. Treatment choice depends on disease type, activity level, overall health, lifestyle, and patient preference. The modern trend favors early use of high-efficacy therapies for better long-term outcomes.
2. Treating Acute Relapses
During severe relapses affecting daily function:
- High-dose corticosteroids (e.g., methylprednisolone) are used short-term to reduce inflammation and speed recovery.
- If steroids fail, plasmapheresis may be used to remove harmful antibodies from the blood.
These treatments do not change the long-term course of the disease.
3. Symptom Management
Symptom control is essential for quality of life and often requires a multidisciplinary approach.
- Fatigue: Energy conservation, cooling strategies, physical therapy, medications such as amantadine or modafinil
- Spasticity: Physical therapy, stretching, baclofen or tizanidine
- Bladder problems: Medications, pelvic floor therapy, or catheterization
- Pain: Anticonvulsants (e.g., gabapentin) or antidepressants
- Cognitive issues: Cognitive rehabilitation and memory strategies
- Depression/anxiety: Psychotherapy and medication
4. The Future of MS Treatment: Promising Research
Current research focuses on two main areas:
- Neuroprotection: Developing drugs that protect nerve fibers from damage.
- Remyelination: Stimulating brain stem cells to repair damaged myelin and restore lost function.
Comprehensive Living With MS: A Holistic Approach
- Psychological and social support are essential after diagnosis.
- Exercise and physical therapy: Regular, appropriate activity reduces fatigue and improves balance and mood.
- Nutrition: A balanced diet rich in vegetables, fruits, and whole grains, with reduced saturated fats and adequate vitamin D.
- Stress management: Meditation, yoga, deep breathing, or time in nature.
- Mental health care: Seeking help from a mental health professional is an important step.
- Regular follow-up with an MS specialist neurologist to monitor disease activity and adjust treatment.
A diagnosis of MS undoubtedly changes a person’s life, but it is no longer what it once was. We have moved from an era of limited options to one with more than 20 disease-modifying therapies, and research is increasingly focused on preventing progression and protecting the nervous system—not just relieving symptoms.
Although every patient’s journey is unique, knowledge, support, specialized care, and a positive approach can make living with MS a life filled with hope and meaning. The future of MS has never been brighter.
To book a consultation or learn about our treatment packages, please contact us or utilize our Online Services. For more updates, visit our Media Center.
Frequently Asked Questions (FAQs) About Multiple Sclerosis
1. What is Multiple Sclerosis (MS)?
MS is an autoimmune and neurodegenerative disease where the body’s immune system mistakenly attacks the protective myelin sheath covering nerve fibers in the central nervous system.
2. What is myelin and why is it important?
Myelin is a fatty layer that insulates nerve fibers, allowing electrical signals from the brain to travel quickly and efficiently to the rest of the body. MS destroys this insulation.
3. What does “Relapsing-Remitting MS” (RRMS) mean?
RRMS is the most common type of MS. It is characterized by clear attacks of symptoms (relapses) followed by periods of partial or complete recovery (remissions) without immediate disease progression.
4. How is Secondary Progressive MS (SPMS) different from RRMS?
Many patients with RRMS eventually transition to SPMS, where the disease begins to progress steadily and neurological function gradually worsens over time, with or without clear relapses.
5. What causes Multiple Sclerosis?
The exact cause is unknown, but it is believed to result from a combination of genetic susceptibility and environmental triggers (such as lack of sunlight, smoking, and prior Epstein-Barr Virus infection).
6. Is Multiple Sclerosis inherited?
MS is not directly hereditary, but genetics play a role. Having a first-degree relative with MS slightly increases your risk compared to the general population.
7. How does Vitamin D affect MS?
Research indicates that low levels of Vitamin D and a lack of sunlight exposure are linked to a higher risk of developing MS, as Vitamin D helps regulate the immune system.
8. What is the most common symptom of MS?
Fatigue is one of the most common and disabling symptoms, affecting about 80% of patients. It is a profound exhaustion that does not improve with simple rest.
9. What is the “MS Hug”?
The “MS hug” is a sensory symptom caused by nerve damage. It feels like a tight band, pressure, or tingling squeezing around the torso or chest.
10. Can MS affect your vision?
Yes. Vision problems, such as optic neuritis (painful, blurred vision), double vision, and involuntary eye movements, are often among the earliest signs of MS.
11. How does MS impact the bladder and bowels?
Nerve damage can cause urinary urgency, frequent urination, incontinence, or incomplete emptying. Bowel issues, primarily constipation, are also common.
12. Is there a single test to diagnose MS?
No single test can definitively diagnose MS. Neurologists rely on medical history, neurological exams, MRI scans, and sometimes a lumbar puncture to rule out other conditions.
13. Why is an MRI important for diagnosing MS?
An MRI can detect characteristic lesions (scarred plaques) in the brain and spinal cord, showing if damage occurred in multiple areas and at different times.
14. What are Oligoclonal bands?
They are abnormal immune proteins found in the cerebrospinal fluid (collected via a lumbar puncture) of over 90% of MS patients, indicating immune activity in the central nervous system.
15. Is there a cure for Multiple Sclerosis?
Currently, there is no cure. However, significant advances have led to over 20 approved medications that can modify the disease course, manage symptoms, and slow progression.
16. What are Disease-Modifying Therapies (DMTs)?
DMTs are medications (injectable, oral, or intravenous) designed to reduce the frequency of relapses, decrease new MRI lesions, and slow the progression of disability.
17. How are acute MS relapses treated?
Severe relapses are usually treated with short courses of high-dose corticosteroids to quickly reduce inflammation. If steroids fail, plasmapheresis (blood filtering) may be used.
18. Does MS cause cognitive problems?
Yes, about 50% of patients experience mild cognitive changes, such as difficulties with short-term memory, concentration, and finding the right words while speaking.
19. What is the future of MS treatment?
Ongoing research is highly promising, focusing on neuroprotection (protecting nerve fibers from damage) and remyelination (stimulating stem cells to repair damaged myelin).
20. Why choose Turkey Healthcare Group for MS management?
We provide access to the best neurologists in Turkey, cutting-edge MRI diagnostics, FDA-approved Disease-Modifying Therapies, and comprehensive physical and psychological rehabilitation programs.
Turkey Healthcare Group stands out with a team of distinguished medical experts in Turkey, who always strive to provide the best healthcare services to patients.
If you are looking for exceptional healthcare or need medical consultation from top doctors, feel free to contact us.
We also invite you to view our leading medical staff and get to know their qualifications and experiences up close.
We are here to ensure you receive the best possible healthcare.